
Everyone is familiar with “OCD”, many people think:
“Always feel like you left the door unlocked and have to go back home to double check?”
“You’ve washed your hands, but you still feel like you’ve got germs?”
“Things have to be neatly organized, and even the slightest misalignment feels unbearable…”
In life, these typical compulsive performance, we will one or two, so say with certainty “I have OCD”!
All of a sudden, OCD has become a fashionable disease, and if you don’t have OCD, it seems that you are out of fashion.
But does compulsive behavior have to be OCD?
The answer is, of course, no!
The real OCD, the extent of far more than popular imagination. Most people say that they are OCD, mistakenly thinking that OCD is a harmless disorder

What is OCD?
Obsessive-compulsive disorder is obsessive-compulsive neurosis, also known as compulsive disorder, it is a kind of mental disorder with repeated persistent compulsive ideas and/or compulsive behavior as the basic characteristics, is a common psychiatric disease.
Studies have found that it is more common in women than men, and most often begins in childhood or early adulthood.
Statistics in recent years suggest that the incidence of OCD is on the rise, with studies showing that the lifetime prevalence of OCD in the general population is 1% to 2%, and about two-thirds of patients develop it before the age of 25.
Obsessive-compulsive disorder because of its early onset, the course of the disease and other characteristics, often have a great impact on the patient’s social function and quality of life.
A global disease survey conducted by the World Health Organization (WHO) found that obsessive-compulsive disorder has become one of the 20 diseases with the highest burden of disease among young and middle-aged people aged 15 to 44.

Obsessive-compulsive disorder clinical manifestation?
The symptoms of obsessive-compulsive disorder can be summarized as compulsive thinking and compulsive behavior.
Obsessive thinking
Persistent and recurring intrusive thoughts (thoughts, impulses, images) that cause significant distress or anxiety, are very distressing to the sufferer, and are difficult to control or eliminate.
Topics of obsessions include primarily harm (e.g., a strong desire to harm oneself or others), cleanliness or contamination (e.g., severe distress over bacterial contamination), and forbidden or taboo thoughts (e.g., aggression or sexual obsessions).
Obsessives can range from repeated doubts about whether Windows and doors are tightly closed, whether you will get sick if you touch something dirty, why the sun rises in the east and sets in the west, to the urge to jump from a balcony.

Obsessives
An action that the patient knows is unreasonable but has to take in order to alleviate the anxiety produced by obsessive thinking.
Such as:
“Patients have doubts about whether the doors and Windows are closed tightly, and will accordingly check the doors and Windows repeatedly to ensure safety;”
“Patients who are afraid of getting sick will wash their hands repeatedly to keep them clean.”

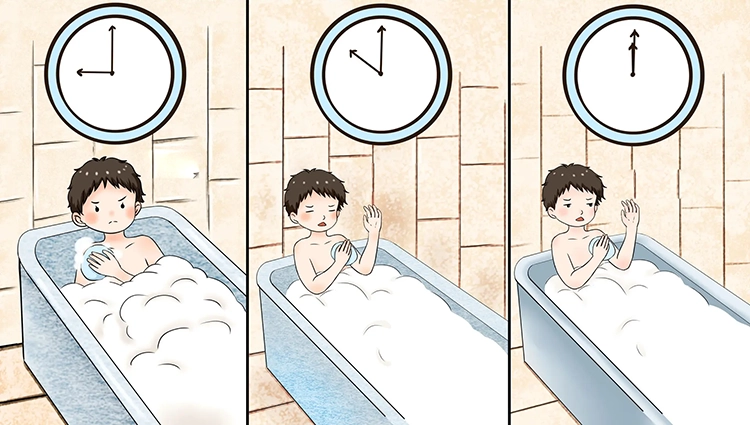
Some patients with a prolonged illness repeat certain movements so often that they develop a routine over time.
When washing hands, it is necessary to wash them from the fingertips and continue to the wrists, and if the order is reversed or interrupted, they must start again, which is often time-consuming and painful.

Obsessive-compulsive symptoms have the following characteristics:
1. It is the patient’s own thinking or impulse, not imposed by the outside world.
2. There must be at least one thought or action that the patient continues to resist in vain, even if the patient no longer resists the other symptoms.
3. The thought of performing the action itself is unpleasant to the sufferer (merely to relieve tension or anxiety is not considered a true pleasure), but if not performed it can produce great anxiety.
4. Thoughts or impulses are unpleasantly recurring.

How does OCD form?
We know that the causes of diseases are often multifactorial and probabilistic, and there is rarely a single cause-and-effect relationship.
Similarly, the causes of OCD are also complex, in order to facilitate understanding, we generally divide the causes of OCD into two types: biological factors and psycho-social factors.

Physiological factors
Heredity:
Obsessive-compulsive disorder has a clear genetic tendency, especially first-degree relatives have compulsion and related disorders, the risk of individual disease is 2-5 times higher, the higher the genetic similarity of family members suffering from obsessive-compulsive disorder the closer the probability.

Neurobiochemical factors:
Some brain nerve damage may cause OCD, such as epilepsy, brain tumor, brain trauma, etc. Some infections and post-infection autoimmune syndrome damage children’s basal ganglia, may cause children to suddenly appear compulsive symptoms.

Psychosocial factors
Personality Traits:
15-35% of patients have compulsive personality traits, such as introversion, timid, serious, indecisive, serious, rigid, conformism, the pursuit of perfection, etc.
Family factors:
Studies have found that people with OCD have a bad family environment, such as low intimacy between family members, lack of commitment and responsibility, and more opposition and conflict.
Inducing factors:
Patients can often be traced back to a variety of stress, frustration, physical illness from daily life, and most of the disease fluctuates in a state of psychological stress.
The common psychological factors of adolescent onset are learning pressure, classmate relationship, love frustration, etc., and parents’ education of their children is too strict, education is inconsistent, etc.

Psychological mechanism
Traditional psychoanalytic schools:
Ocd is the result of the interaction of psychological conflict and psychological defense mechanisms, and patients often have certain mental trauma in their early life experiences;
Behaviorist school:
The form of obsessive-compulsive symptoms is the result of the classical conditioning that makes up the anxiety response and the operational conditioning of the obsessive action or behavior;
Theories of cognitive psychology:
The occurrence of negative automatic thoughts that cause negative emotions when recurring intrusive thoughts interact with his belief system (such as absolutism, excessive sense of responsibility, perfectionist demands, and exaggerated danger imagination);

Humanistic doctrine:
Lacking the need for security, they do not trust themselves or the outside world, and in order to avoid fear, they arrange their world to be predictable and controllable.